Training Logbook
| Part of | Uniplanar External Fixation |
|---|---|
| Required time | 30-45 minutes |

This module allows medical officers, junior orthopedic surgery residents, and surgeons who are not orthopedic specialists to become confident and competent in irrigation and debridement, powered and manual drilling, positioning and correctly inserting Schanz screws, and constructing the uniplanar external fixator frame as part of external fixation procedures for open tibial shaft fractures performed in regions without specialist coverage. To maximize patient safety, this module teaches learners to use a powered drill to insert self-drilling Schanz screws through the near cortex and then manually advance Schanz screws into the far cortex to avoid plunging.
Training Logbook
Sterile Prepping and Draping
Date of Procedure (month, day, year):__________________
Procedure Start Time:__________________AM;____________________PM
| # | Checklist for Simulation-Based Skills Training Procedure and Self-Assessment Framework | Check the most appropriate response |
|---|---|---|
| 1 | Place simulated patient in the supine position | Done Correctly
Done Incorrectly Not Done |
| 2 | Directed assistant #1 to use both gloved hands to support the simulated patient's foot to lift up the injured leg | Done Correctly
Done Incorrectly Not Done |
| 3 | The surgical practitioner used a sponge stick and folded up gauze pad to simulate the circumferential prepping of the injured leg three times in a distal-to-proximal direction from below the ankle to the mid-thigh | Done Correctly
Done Incorrectly Not Done |
| 4A | While the prepped leg was held up by assistant #1, the surgical practitioner and assistant #2 placed the first drape on the inferior (caudal) section of the simulated operating table to cover the simulated patient's contralateral leg and the simulated operating table underneath the patient's prepped leg to above the mid-thigh region | Done Correctly
Done Incorrectly Not Done |
| 4B | While the prepped leg was held up by assistant #1, the surgical practitioner and assistant #2 placed a second drape over the first drape, wrapped the superior (cephalad) section of this second drape underneath and over the mid-thigh of the prepped leg, and secured this wrapped drape with a towel clamp over the anterior aspect of the leg | Done Correctly
Done Incorrectly Not Done |
| 4C | While the prepped leg was held up by assistant #1, the surgical practitioner and assistant #2 placed a third drape over the superior (cephalad) section of the simulated operating table to cover the patient's body from the mid-thigh to the torso, wrapped the inferior (caudal) section of the third drape over and underneath the mid-thigh of the prepped leg, and secured this wrapped drape with a towel clamp over the lateral aspect of the leg | Done Correctly
Done Incorrectly Not Done |
| 4D | While the prepped leg was held up by assistant #1, the surgical practitioner placed a towel centred underneath the patient's foot on the second drape | Done Correctly
Done Incorrectly Not Done |
| 5 | The assistant #1 gently lowered the foot onto this towel | Done Correctly
Done Incorrectly Not Done |
| 6 | The surgical practitioner wrapped this towel around and over the patient's foot to cover the entire foot to just above the ankle, and secured this towel with a towel clamp | Done Correctly
Done Incorrectly Not Done |
| 7 | The surgical practitioner wrapped a roll of gauze around the wrapped foot to help ensure the towel does not slip off and then secured the gauze by tucking the end of the gauze underneath itself | Done Correctly
Done Incorrectly Not Done |
| 8 | Were all the Training Logbook checklist items rated as "Done Correctly"? | YesNo |
Learner's Name:____________________________________
Assistant's Name:____________________________________
Procedure End Time:__________________AM;____________________PM
Total Procedure Time (Procedure End Time - Procedure Start Time):__________________
Uniplanar External Fixation for an Open Tibial Shaft Transverse Fracture
Date of Procedure (month, day, year):__________________
Procedure Start Time:__________________AM;____________________PM
| # | Checklist for Simulation-Based Skills Training Procedure and Self-Assessment Framework | Check the most appropriate response |
|---|---|---|
| 1A | Wore proper eye protection and gloves |
Done Correctly Done Incorrectly Not Done |
| 1B | Loosened the right vise clamp securing the distal fragment to simulate a displaced fracture during this simulation-based skills training |
Done Correctly Done Incorrectly Not Done |
| 1C | Performed simulated irrigation using an average of 3L of irrigation solution for each successive Gustilo Type (i.e., 6L for Gustilo Type II open tibial fracture and 9L for Gustilo Type III open tibial fracture) to reduce the risk of infection |
Done Correctly Done Incorrectly Not Done |
| 1D | Debrided all foreign material and non-viable tissue to prevent infection and minimize wound complications | This Step Cannot Be Performed During This Simulation-Based Skills Training But Must Be Performed During the Actual Clinical Procedure |
| 2A | If required, extended the open wound to directly visualize the fracture | This Step Cannot Be Performed During This Simulation-Based Skills Training But Must Be Performed During the Actual Clinical Procedure |
| 2B | While directly visualizing the fracture, applied manual longitudinal traction to the distal lower extremity to reduce the fracture | This Step Cannot Be Performed During This Simulation-Based Skills Training But Must Be Performed During the Actual Clinical Procedure |
| 2C | Used bone reduction forceps to manually reduce the fracture, compress the fragments together, and restore alignment:
Bone apposition > 50% Rotation < 10 degrees Angulation < 10 degrees in any plane Length discrepancy < 2 cm shortening No distraction (lengthening) |
Done Correctly Done Incorrectly Not Done |
| 2D | Confirmed restoration of rotational alignment by visually checking the position of the big toe and the alignment of the middle of the second toe with the center of the patella:
|
This Step Cannot Be Performed During This Simulation-Based Skills Training But Must Be Performed During the Actual Clinical Procedure |
| 2E | Palpated the medial malleolus of both limbs under sterile conditions to estimate and compare the length of the reduced limb to the uninjured limb:
|
This Step Cannot Be Performed During This Simulation-Based Skills Training But Must Be Performed During the Actual Clinical Procedure |
| 2F | Applied bone holding forceps to maintain the reduced fracture |
Done Correctly Done Incorrectly Not Done |
| 2G | Tightened right vise clamp and removed bone reduction forceps once fracture is stabilized during this simulation-based skills training |
Done Correctly Done Incorrectly Not Done |
| 3A | Positioned the “far” Schanz screw (furthest from the fracture line) in the proximal fragment in the anteromedial tibial wall medial or distal to the tibial tuberosity while avoiding traumatized soft tissues to avoid tethering of the patellar ligament and penetration into the knee joint |
Done Correctly Done Incorrectly Not Done |
| 3B | Used a 22 blade scalpel to make a stab incision for insertion of the Schanz screw in the soft tissue (not shown) overlying the anteromedial tibial wall and not on the tibial crest to reduce the risk of thermal osteonecrosis and reduce the risk that the screw tip may slip and injure the soft tissues during drilling | This Step Cannot Be Performed During This Simulation-Based Skills Training But Must Be Performed During the Actual Clinical Procedure |
| 3C | Used dissecting scissors to spread the soft tissue (not shown) apart in the stab incision to expose the bone for drilling of the Schanz screw | This Step Cannot Be Performed During This Simulation-Based Skills Training But Must Be Performed During the Actual Clinical Procedure |
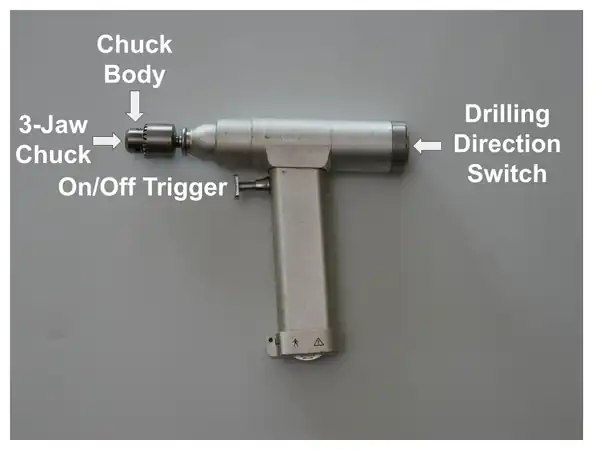
| 3D | Prepared the powered surgical drill for use by placing the Schanz screw into the 3-jaw chuck, inserting the chuck key into the circular opening in the chuck body, turning the chuck key clockwise to tighten the 3-jaw chuck over the Schanz screw, and then engaging the switch for forward drilling direction
|
Done Correctly Done Incorrectly Not Done |
| 3E | Confirmed that the drill is ready for use by pressing the on/off trigger and observing that the Schanz screw tip is rotating clockwise when the drill is pointing forward |
Done Correctly Done Incorrectly Not Done |
| 3F | Placed the properly sized drill sleeve directly on the near cortex in the stab incision to protect the surrounding soft tissues when drilling |
Done Correctly Done Incorrectly Not Done |
| 3G | Slid the Schanz screw into the properly sized drill sleeve and placed the screw tip directly on the near cortex of the anteromedial tibial wall and not on the tibial crest to reduce the risk of thermal osteonecrosis and reduce the risk that the screw tip may slip and injure the soft tissues during drilling | Done Correctly
Done Incorrectly Not Done |
| 3H | Inserted the "far" Schanz screw in the proximal fragment at a drill trajectory angle between 30°-60° relative to the tibial crest to avoid injury to neurovascular structures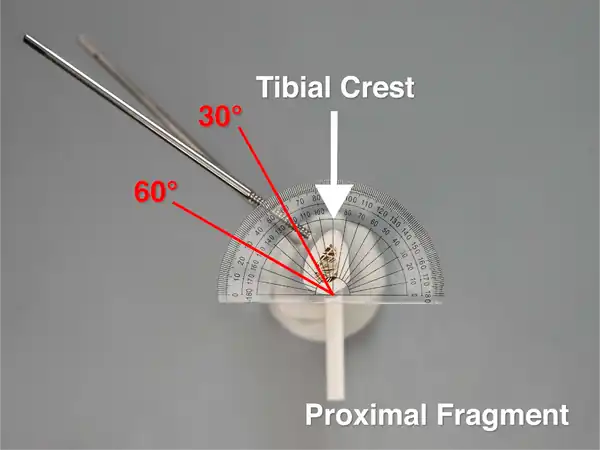
|
Done Correctly Done Incorrectly Not Done |
| 3I | Pulled back and kept the properly sized drill sleeve at least 3.0 mm above the near cortex only during this simulation-based skills training to prevent plastic strands from getting stuck inside the drill sleeve while drilling | Done Correctly
Done Incorrectly Not Done |
| 3J | Directed an assistant to perform simulated irrigation while drilling to reduce the risk of thermal osteonecrosis |
Done Correctly Done Incorrectly Not Done |
| 3K | Started drilling with the Schanz screw tip rotating in a clockwise direction and ensured that the tip did not slip medially or laterally on the near cortex which could injure the soft tissues |
Done Correctly Done Incorrectly Not Done |
| 3L | Power drilled the Schanz screw through the near cortex of the anteromedial tibial wall and used tactile feel and acoustic feedback to stop drilling after passing through the near cortex and before or when the inner surface of the far cortex is reached to avoid plunging through the far cortex and damaging underlying soft tissues |
Done Correctly Done Incorrectly Not Done |
| 3M | Inserted the chuck key into the circular opening in the drill chuck body, turned the chuck key anticlockwise, detached the drill and removed the drill sleeve from the Schanz screw |
Done Correctly Done Incorrectly Not Done |
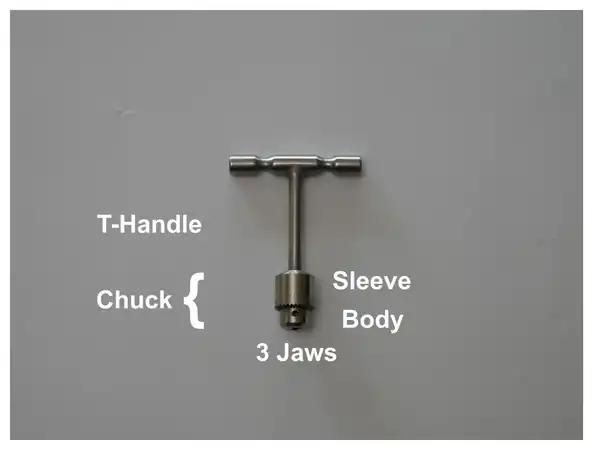
| 3N | Slid the universal chuck with T-handle over the Schanz screw and tightened the 3-jaw chuck over the Schanz screw by manually rotating the chuck sleeve clockwise or by inserting the chuck key into the circular opening in the chuck body and turning the chuck key clockwise
|
Done Correctly Done Incorrectly Not Done |
| 3O | Used the universal chuck with T-handle to turn the Schanz screw manually for one to two 360 degree rotations to anchor the screw tip into the far cortex without exiting the far cortex to avoid injuring underlying soft tissue |
Done Correctly Done Incorrectly Not Done |
| 3P | Detached the universal chuck with T-handle from the Schanz screw by manually rotating the chuck sleeve anticlockwise or by inserting the chuck key into the circular opening in the chuck body and turning the chuck key anticlockwise |
Done Correctly Done Incorrectly Not Done |
| 4A | Placed the "far" Schanz screw (furthest from the fracture line) in the distal fragment in the anteromedial tibial wall at least 2 fingers’ breadth proximal to the medial malleolus (not shown) while avoiding traumatized soft tissues to avoid entry into the ankle join | This Step Cannot Be Performed During This Simulation-Based Skills Training But Must Be Performed During the Actual Clinical Procedure |
| 4B | Positioned the 2 “far” Schanz screws as widely spaced as possible into each fragment while avoiding traumatized soft tissues and entry into knee and ankle joints to permit better control of displacing forces and optimize stabilization of the reduction |
Done Correctly Done Incorrectly Not Done |
| 4C | Used a 22 blade scalpel to make a stab incision for insertion of the Schanz screw in the soft tissue (not shown) overlying the anteromedial tibial wall and not on the tibial crest to reduce the risk of thermal osteonecrosis and reduce the risk that the screw tip may slip and injure the soft tissues during drilling | This Step Cannot Be Performed During This Simulation-Based Skills Training But Must Be Performed During the Actual Clinical Procedure |
| 4D | Used dissecting scissors to spread the soft tissue (not shown) apart in the stab incision to expose the bone for drilling of the Schanz screw | This Step Cannot Be Performed During This Simulation-Based Skills Training But Must Be Performed During the Actual Clinical Procedure |
| 4E | Placed the Schanz screw into the 3-jaw chuck of the powered surgical drill, inserted the chuck key into the circular opening in the chuck body, turned the chuck key clockwise to tighten the 3-jaw chuck over the Schanz screw, and then engaged the switch for forward drilling |
Done Correctly Done Incorrectly Not Done |
| 4F | Confirmed that the drill is ready for use by pressing the on/off trigger and observing that the Schanz screw tip is rotating clockwise when the drill is pointing forward |
Done Correctly Done Incorrectly Not Done |
| 4G | Placed the properly sized drill sleeve directly on the near cortex in the stab incision to protect the surrounding soft tissues when drilling |
Done Correctly Done Incorrectly Not Done |
| 4H | Slid the Schanz screw into the properly sized drill sleeve and placed the screw tip directly on the near cortex of the anteromedial tibial wall and not on the tibial crest to reduce the risk of thermal osteonecrosis and reduce the risk that the screw tip may slip and injure the soft tissues during drilling | Done Correctly
Done Incorrectly Not Done |
| 4I | Inserted the "far" Schanz screw in the distal fragment at an identical drill trajectory angle to the "far" Schanz screw in the proximal fragment and between 30°-60° relative to the tibial crest to avoid injury to neurovascular structures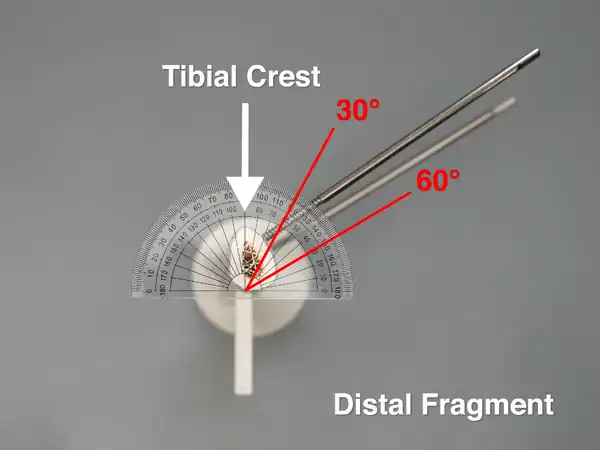
|
Done Correctly Done Incorrectly Not Done |
| 4J | Pulled back and kept the properly sized drill sleeve at least 3.0 mm above the near cortex only during this simulation-based skills training to prevent plastic strands from getting stuck inside the drill sleeve while drilling | Done Correctly
Done Incorrectly Not Done |
| 4K | Directed an assistant to perform simulated irrigation while drilling to reduce the risk of thermal osteonecrosis |
Done Correctly Done Incorrectly Not Done |
| 4L | Started drilling with the Schanz screw tip rotating in a clockwise direction and ensured that the tip did not slip medially or laterally on the near cortex which could injure the soft tissues |
Done Correctly Done Incorrectly Not Done |
| 4M | Power drilled the Schanz screw through the near cortex of the anteromedial tibial wall and used tactile feel and acoustic feedback to stop drilling after passing through the near cortex and before or when the inner surface of the far cortex is reached to avoid plunging through the far cortex and damaging underlying soft tissues |
Done Correctly Done Incorrectly Not Done |
| 4N | Inserted the chuck key into the circular opening in the drill chuck body, turned the chuck key anticlockwise, detached the drill and removed the drill sleeve from the Schanz screw |
Done Correctly Done Incorrectly Not Done |
| 4O | Slid the universal chuck with T-handle over the Schanz screw and tightened the 3-jaw chuck over the Schanz screw by manually rotating the chuck sleeve clockwise or by inserting the chuck key into the circular opening in the chuck body and turning the chuck key clockwise |
Done Correctly Done Incorrectly Not Done |
| 4P | Used the universal chuck with T-handle to turn the Schanz screw manually for one to two 360 degree rotations to anchor the screw tip into the far cortex without exiting the far cortex to avoid injuring underlying soft tissues |
Done Correctly Done Incorrectly Not Done |
| 4Q | Detached the universal chuck with T-handle from the Schanz screw by manually rotating the chuck sleeve anticlockwise or by inserting the chuck key into the circular opening in the chuck body and turning the chuck key anticlockwise |
Done Correctly Done Incorrectly Not Done |
| 5A | Inserted 4 pin-to-rod clamps on a 300 mm uniplanar rod and applied the 2 outer pin-to-rod clamps to connect the 2 "far" Schanz screws in each fragment to the 300 mm rod |
Done Correctly Done Incorrectly Not Done |
| 5B | Tightened the 2 outer pin-to-rod clamps initially by hand and left the 2 inner pin-to-rod clamps loosened |
Done Correctly Done Incorrectly Not Done |
| 6A | Placed the “near” Schanz screw (closest to the fracture line) at least 2.0 cm (a finger breadth) from the fracture line while avoiding traumatized soft tissues to help prevent the placement of the Schanz screw within the fracture hematoma and risk having a pin site infection spread within the fracture and positioned the "near" and "far" Schanz screws as widely spaced as possible in each fragment to permit better control of displacing forces and optimize stabilization of the reduction |
Done Correctly Done Incorrectly Not Done |
| 6B | Used a 22 blade scalpel to make a stab incision for insertion of the Schanz screw in the soft tissue (not shown) overlying the anteromedial tibial wall and not on the tibial crest to reduce the risk of thermal osteonecrosis and reduce the risk that the screw tip may slip and injure the soft tissues during drilling | This Step Cannot Be Performed During This Simulation-Based Skills Training But Must Be Performed During the Actual Clinical Procedure |
| 6C | Used dissecting scissors to spread the soft tissue (not shown) apart in the stab incision to expose the bone for drilling of the Schanz screw | This Step Cannot Be Performed During This Simulation-Based Skills Training But Must Be Performed During the Actual Clinical Procedure |
| 6D | Placed the Schanz screw into the 3-jaw chuck of the powered surgical drill, inserted the chuck key into the circular opening in the chuck body, turned the chuck key clockwise to tighten the 3-jaw chuck over the Schanz screw, and then engaged the switch for forward drilling |
Done Correctly Done Incorrectly Not Done |
| 6E | Confirmed that the drill is ready for use by pressing the on/off trigger and observing that the Schanz screw tip is rotating clockwise when the drill is pointing forward |
Done Correctly Done Incorrectly Not Done |
| 6F | Inserted the "near" Schanz screw into the loosened pin opening in the rod-to-pin clamp attached to the 300 mm rod |
Done Correctly Done Incorrectly Not Done |
| 6G | Placed the Schanz screw tip directly on the near cortex of the anteromedial tibial wall and not on the tibial crest to reduce the risk of thermal osteonecrosis and reduce the risk that the screw tip may slip and injure the soft tissues during drilling |
Done Correctly Done Incorrectly Not Done |
| 6H | Inserted the "near" Schanz screw at an identical drill trajectory angle to all the other Schanz screws and between 30°-60° relative to the tibial crest to avoid injury to neurovascular structures |
Done Correctly Done Incorrectly Not Done |
| 6I | Directed an assistant to perform simulated irrigation while drilling to reduce the risk of thermal osteonecrosis |
Done Correctly Done Incorrectly Not Done |
| 6J | Started drilling with the Schanz screw tip rotating in a clockwise direction and ensured that the tip did not slip medially or laterally on the near cortex which could injure the soft tissues |
Done Correctly Done Incorrectly Not Done |
| 6K | Power drilled the Schanz screw through the near cortex of the anteromedial tibial wall and used tactile feel and acoustic feedback to stop drilling after passing through the near cortex and before or when the inner surface of the far cortex is reached to avoid plunging through the far cortex and damaging underlying soft tissues |
Done Correctly Done Incorrectly Not Done |
| 6L | Inserted the chuck key into the circular opening in the drill chuck body, turned the chuck key anticlockwise, and removed the drill from the Schanz screw |
Done Correctly Done Incorrectly Not Done |
| 6M | Slid the universal chuck with T-handle over the Schanz screw and tightened the 3-jaw chuck over the Schanz screw by manually rotating the chuck sleeve clockwise or by inserting the chuck key into the circular opening in the chuck body and turning the chuck key clockwise |
Done Correctly Done Incorrectly Not Done |
| 6N | Used the universal chuck with T-handle to turn the Schanz screw manually for one to two 360 degree rotations to anchor the screw tip into the far cortex without exiting the far cortex to avoid injuring underlying soft tissues |
Done Correctly Done Incorrectly Not Done |
| 6O | Detached the universal chuck with T-handle from the Schanz screw by manually rotating the chuck sleeve anticlockwise or by inserting the chuck key into the circular opening in the chuck body and turning the chuck key anticlockwise |
Done Correctly Done Incorrectly Not Done |
| 7A | Placed the “near” Schanz screw (closest to the fracture line) at least 2.0 cm (a finger breadth) from the fracture line while avoiding traumatized soft tissues to help prevent the placement of the Schanz screw within the fracture hematoma and risk having a pin site infection spread within the fracture and positioned the "near" and "far" Schanz screws as widely spaced as possible in each fragment to permit better control of displacing forces and optimize stabilization of the reduction |
Done Correctly Done Incorrectly Not Done |
| 7B | Used a 22 blade scalpel to make a stab incision for insertion of the Schanz screw in the soft tissue (not shown) overlying the anteromedial tibial wall and not on the tibial crest to reduce the risk of thermal osteonecrosis and reduce the risk that the screw tip may slip and injure the soft tissues during drilling | This Step Cannot Be Performed During This Simulation-Based Skills Training But Must Be Performed During the Actual Clinical Procedure |
| 7C | Used dissecting scissors to spread the soft tissue (not shown) apart in the stab incision to expose the bone for drilling of the Schanz screw | This Step Cannot Be Performed During This Simulation-Based Skills Training But Must Be Performed During the Actual Clinical Procedure |
| 7D | Placed the Schanz screw into the 3-jaw chuck of the powered surgical drill, inserted the chuck key into the circular opening in the chuck body, turned the chuck key clockwise to tighten the 3-jaw chuck over the Schanz screw, and then engaged the switch for forward drilling |
Done Correctly Done Incorrectly Not Done |
| 7E | Confirmed that the drill is ready for use by pressing the on/off trigger and observing that the Schanz screw tip is rotating clockwise when the drill is pointing forward |
Done Correctly Done Incorrectly Not Done |
| 7F | Inserted the "near" Schanz screw into the loosened pin opening in the rod-to-pin clamp attached to the 300 mm rod |
Done Correctly Done Incorrectly Not Done |
| 7G | Placed the Schanz screw tip directly on the near cortex of the anteromedial tibial wall and not on the tibial crest to reduce the risk of thermal osteonecrosis and reduce the risk that the screw tip may slip and injure the soft tissues during drilling |
Done Correctly Done Incorrectly Not Done |
| 7H | Inserted the "near" Schanz screw at an identical drill trajectory angle to all the other Schanz screws and between 30°-60° relative to the tibial crest to avoid injury to neurovascular structures |
Done Correctly Done Incorrectly Not Done |
| 7I | Directed an assistant to perform simulated irrigation while drilling to reduce the risk of thermal osteonecrosis |
Done Correctly Done Incorrectly Not Done |
| 7J | Started drilling with the Schanz screw tip rotating in a clockwise direction, and ensured that the tip did not slip medially or laterally on the near cortex which could injure the soft tissues |
Done Correctly Done Incorrectly Not Done |
| 7K | Power drilled the Schanz screw through the near cortex of the anteromedial tibial wall and used tactile feel and acoustic feedback to stop drilling after passing through the near cortex and before or when the inner surface of the far cortex is reached to avoid plunging through the far cortex and damaging underlying soft tissues |
Done Correctly Done Incorrectly Not Done |
| 7L | Inserted the chuck key into the circular opening in the drill chuck body, turned the chuck key anticlockwise, and removed the drill from the Schanz screw |
Done Correctly Done Incorrectly Not Done |
| 7M | Slid the universal chuck with T-handle over the Schanz screw and tightened the 3-jaw chuck over the Schanz screw by manually rotating the chuck sleeve clockwise or by inserting the chuck key into the circular opening in the chuck body and turning the chuck key clockwise |
Done Correctly Done Incorrectly Not Done |
| 7N | Used the universal chuck with T-handle to turn the Schanz screw manually for one to two 360 degree rotations to anchor the screw tip into the far cortex without exiting the far cortex to avoid injuring underlying soft tissues |
Done Correctly Done Incorrectly Not Done |
| 7O | Detached the universal chuck with T-handle from the Schanz screw by manually rotating the chuck sleeve anticlockwise or by inserting the chuck key into the circular opening in the chuck body and turning the chuck key anticlockwise |
Done Correctly Done Incorrectly Not Done |
| 8A | Applied and turned the 11 mm spanner with T-handle wrench clockwise for final tightening of the 4 pin-to-rod clamps |
Done Correctly Done Incorrectly Not Done |
| 8B | Verified the reduction visually, and with gentle palpation of the tibial crest at the fracture line to confirm that the alignment is still within acceptable parameters:
Bone apposition > 50% Rotation < 10 degrees Angulation < 10 degrees in the coronal (frontal) and sagittal planes |
Done Correctly Done Incorrectly Not Done |
| 8C | Visually checked the position of the big toe and the alignment of the middle of the second toe with the center of patella to confirm whether rotational alignment is still adequately restored:
|
This Step Cannot Be Performed During This Simulation-Based Skills Training But Must Be Performed During the Actual Clinical Procedure |
| 8D | Visually inspected the fracture line to confirm that the reduction is adequate during this simulation-based skills training:
Length discrepancy < 2 cm shortening No distraction (lengthening) |
Done Correctly Done Incorrectly Not Done |
| 8E | Palpated the medial malleolus of both limbs under sterile conditions to estimate and compare the length of the reduced limb to the uninjured contralateral limb:
|
This Step Cannot Be Performed During This Simulation-Based Skills Training But Must Be Performed During the Actual Clinical Procedure |
| 8F | Removed the bone holding forceps once the reduced fracture is stabilized with the external fixator frame and acceptable alignment is confirmed | Done Correctly
Done Incorrectly Not Done |
| 8G | Checked for skin tenting around Schanz screws and if present, widened the stab incision to release soft tissue tension around the pin site to reduce the risk of inflammation and pin site infection | This Step Cannot Be Performed During This Simulation-Based Skills Training But Must Be Performed During the Actual Clinical Procedure |
| 8H | Cleaned the extremity and applied sterile gauze dressings to all 4 pin sites at the end of the procedure | This Step Cannot Be Performed During This Simulation-Based Skills Training But Must Be Performed During the Actual Clinical Procedure |
| 8I | Used a measuring tape to measure and compare the limb length (from anterior superior iliac spine to the medial malleolus) of both legs after dressings have been applied:
|
This Step Cannot Be Performed During This Simulation-Based Skills Training But Must Be Performed During the Actual Clinical Procedure |
| 8J | Re-evaluated the Gustilo open-fracture classification for the open tibial shaft fracture in the operating room and updated the antibiotic regimen and surgical treatment plan accordingly | This Step Cannot Be Performed During This Simulation-Based Skills Training But Must Be Performed During the Actual Clinical Procedure |
| 8K | Provided specific, clear, and concise directions to the assistant during this simulation-based skills training |
Done Correctly Done Incorrectly Not Done |
| 9A | Took an anterior view photo of the simulator with a ruler in the image to provide scale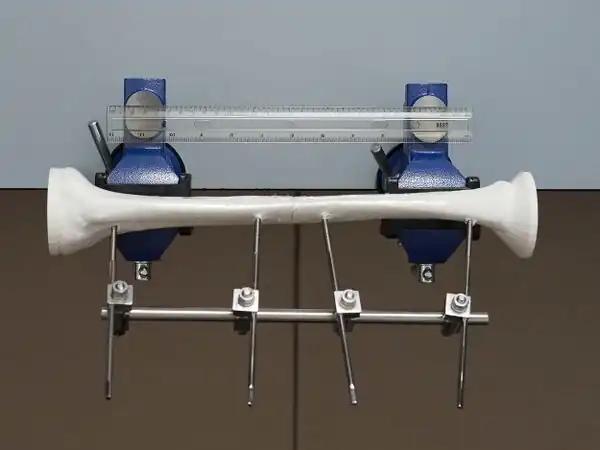
|
Done Correctly Done Incorrectly Not Done |
| 9B | Visually inspected the tibial shaft in the anterior photo and confirmed that alignment is within acceptable parameters:
Bone apposition > 50% Rotation < 10 degrees Angulation < 10 degrees in the coronal plane |
Done Correctly Done Incorrectly Not Done |
| 9C | Used the ruler to measure the distance of the 2 "near" Schanz screws from the fracture line |
Done Correctly Done Incorrectly Not Done |
| 9D | The 2 "near" Schanz screws were placed at least 2.0 cm (a finger breadth) from the fracture line to help prevent the placement of the Schanz screw within the fracture hematoma and reduce the risk of having a pin site infection spread within the fracture |
Done Correctly Done Incorrectly Not Done |
| 9E | Visually inspected the fracture line to confirm that the reduction is adequate:
Length discrepancy < 2 cm shortening No distraction (lengthening) |
Done Correctly Done Incorrectly Not Done |
| 9F | Took a medial view photo of the simulator |
Done Correctly Done Incorrectly Not Done |
| 9G | The "far" Schanz screw in the proximal fragment was inserted medial or distal to the tibial tuberosity to avoid tethering of the patellar ligament and penetration into the knee joint |
Done Correctly Done Incorrectly Not Done |
| 9H | All 4 Schanz screws were inserted medial to the tibial crest in the medial photo to reduce the risk of thermal osteonecrosis and reduce the risk that the screw tip may slip and injure the soft tissues |
Done Correctly Done Incorrectly Not Done |
| 9I | Took a lateral view photo of the simulator
|
Done Correctly Done Incorrectly Not Done |
| 9J | All 4 Schanz screws in the lateral photo did not perforate the far cortex to avoid injuring underlying soft tissues |
Done Correctly Done Incorrectly Not Done |
| 9K | Visually inspected the tibial crest in the lateral photo and confirmed that alignment is within acceptable parameters:
Bone apposition > 50% Rotation < 10 degrees Angulation < 10 degrees in the sagittal plane |
Done Correctly Done Incorrectly Not Done |
| 9L | Removed the rods and clamps but left the 4 Schanz screws in the distal and proximal fragments, used scissors to cut the cellophane wrap overlying the fracture site to separate the 2 fragments, removed each fragment from the vise clamp, and placed each fragment on a flat surface for inspection of the drill trajectory angles
|
Done Correctly Done Incorrectly Not Done |
| 9M | Placed a protractor on the cross-section of the proximal fragment and lined up the center vertical black line of the protractor with the center of the vise attachment |
Done Correctly Done Incorrectly Not Done |
| 9N | Took an overhead ("bird's eye view") photo of the cross-section of the proximal fragment to record the drill trajectory angles relative to the tibial crest and verified that the center vertical black line of the protractor was lined up with the center of the vise attachment
|
Done Correctly Done Incorrectly Not Done |
| 9O | For the proximal fragment, the drill trajectory angles of both Schanz screws are identical and between 30°-60° relative to the tibial crest to avoid injury to neurovascular structures |
Done Correctly Done Incorrectly Not Done |
| 9P | Placed a protractor on the cross-section of the distal fragment and lined up the center vertical black line of the protractor with the center of the vise attachment |
Done Correctly Done Incorrectly Not Done |
| 9Q | Took an overhead ("bird's eye view") photo of the cross-section of the distal fragment to record the drill trajectory angles relative to the tibial crest and verified that the center vertical black line of the protractor was lined up with the center of the vise attachment
|
Done Correctly Done Incorrectly Not Done |
| 9R | For the distal fragment, the drill trajectory angles of both Schanz screws are identical and between 30°-60° relative to the tibial crest to avoid injury to neurovascular structures |
Done Correctly Done Incorrectly Not Done |
| 9S | The drill trajectory angles of the 4 Schanz screws inserted into the proximal and distal fragments are identical |
Done Correctly Done Incorrectly Not Done |
| 9T | Saved all 5 self-assessment framework photos of the simulator on the learner's cellphone for their training records |
Done Correctly Done Incorrectly Not Done |
| 10 | Were all the Training Logbook checklist items (except for the steps that cannot be performed during this simulation-based skills training) rated as "Done Correctly"? |
Yes No |
Learner's Name:____________________________________
Assistant's Name:____________________________________
Procedure End Time:__________________AM;____________________PM
Total Procedure Time (Procedure End Time - Procedure Start Time):__________________
Creating a PDF for Training Records
After clicking on the appropriate checkboxes on this page, here's how to create a PDF document that can be saved on the learner's mobile device or computer for their training records.
Android System
- On your Android device, open the Chrome app.[1][2]
- Open this page and click to check the appropriate checkboxes.
- At the top right, tap "More" (the three-dot button) and then "Share."
- Select "Print."
- At the top right, tap the Down arrow and choose "Save as PDF" from the options menu.
- At right, tap the blue PDF button to save your PDF to an appropriate folder (i.e., Downloads).
iOS System
- On your iPhone or iPad, open the Chrome app.[3]
- Open this page and click to check the appropriate checkboxes.
- At the top right, tap "Share" (box with an upward arrow).
- Select "Print."
- On the Options page, tap "Share" (box with an upward arrow) at the top right.
- Select "Save to Files" and "Save" PDF to an appropriate folder (i.e., Downloads).
Laptop or Desktop Computer
- On your computer, open the Chrome app.[4]
- Open this page and click to check the appropriate checkboxes.
- Click "File" and then "Print." Or, use a keyboard shortcut (Windows & Linux: "Ctrl + p"; Mac: "⌘ + p"). Or, click on the 3 vertical dots at the top right and select "Print."
- For "Destination," select "Save as PDF" and "Save" PDF to an appropriate folder (i.e., Downloads).
Acknowledgements
This work is funded by a grant from the Intuitive Foundation. Any research, findings, conclusions, or recommendations expressed in this work are those of the author(s), and not of the Intuitive Foundation.
References
- ↑ https://support.google.com/chrome/answer/1069693?hl=en&co=GENIE.Platform%3DAndroid&oco=0
- ↑ https://www.tomsguide.com/how-to/how-to-save-a-web-page-as-a-pdf
- ↑ https://support.google.com/chrome/answer/1069693?hl=en&co=GENIE.Platform%3DiOS
- ↑ https://support.google.com/chrome/answer/1069693?hl=en&co=GENIE.Platform%3DDesktop&oco=0
| Authors | Medical Makers, Habila Umaru |
|---|---|
| License | CC-BY-SA-4.0 |
| Organizations | Medical Makers |
| Cite as | Medical Makers, Habila Umaru (2022–2025). "Uniplanar External Fixation/Training Logbook". Appropedia. Retrieved November 28, 2025. |